Testosterone Phenylpropionate
Cas No 1255-49-8
Chemical Formulas
C9H10O2
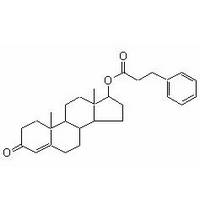
Chemical Name: Testosterone
Phenylpropionate
Drug Class: Injectable Anabolic Steroid
Synonyms: Retandrol, Testolent, Testosterone phenylpropionate,
Testosterone phenpropionate, Testosterone, hydrocinnamate,
Testosterone 17-phenylpropionate, Testosterone hydrocinnamate,
T9890_SIGMA, EINECS 215-014-4, NSC 26643, BB_NC-0581, NSC26643,
TESTOSTERONE PHENYL PROPIONATE, ZINC03881605,
17beta-Hydroxyandrost-4-en-3-one 3-phenylpropionate, LS-148821,
C14667, 4-Androsten-17beta-ol-3-one 17-phenylpropionate, 1255-49-8,
Androst-4-en-3-one, 17-(1-oxo-3-phenylpropoxy)-, (17-beta)-Phenylpropoxy)-,
(17-beta)
|
Molecular Formula:
|
C28H36O3 |
Molecular Weight:
|
420.583640 [g/mol] |
|
H-Bond Donor:
|
0 |
H-Bond Acceptor:
|
3 |
InChIKey: HHSXYDOROIURIP-FEZCWRLCSA-N
Chemical data
Formula C9H10O2
Testosterone phenylpropionate is a slow-acting ester, with a release
time of 1-3 weeks. A popular name brand for T-phenylpropionate is "Testolent."
Testosterone phenylpropionate is also one of the components of
Sustanon and Omnadren.
Testosterone is a hormone
produced predominantly in the testes of males. It is responsible for
nearly all of the sexual traits in males. This specific version is
Testosterone with the Phenylpropionate ester attached. It has an
active life of 4-5 day. Release time-wise, it is directly in the
middle of the Propionate (short) and Cypionate (long) versions of
Testosterone. It is recommended to inject this version two times per
week, although many prefer every third day.
Background
Testosterone was first synthesized by being isolated from bulls’
testicles in 1935. Many pharmaceutical forms and derivatives have
been created since.
This version of Testosterone was originally manufactured by the
Sicomed Pharmaceutical house under the brand name, “Testolent.” For
many years, Testosterone Phenylpropionate was difficult to obtain
but has recently been made more available by underground labs.
Steroid Action
Testosterone is responsible for promoting health and well-being
through enhanced libido, energy, immunity, increased fat loss,
gaining and maintaining lean musc le mass, preventing Osteoporosis
(loss of bone density) and possible protection against heart
disease. Testosterone is also responsible for normal growth and
development of male sex organs and maintenance of secondary sex
characteristics. Secondary sex characteristics are specific traits
that separate the two sexes, but are not directly part of the
reproductive system, for example: chest and facial hair, a
distinguished jaw line, broad shoulders and increased muscle mass.
Testosterone binds to the Androgen Receptors (AR), which thus causes
accelerated muscle gain, fat loss, and muscle repair and growth.
These mechanisms are stimulated by activation of the Androgen
Receptors (either directly or as DHT). le mass, preventing Osteoporosis
(loss of bone density) and possible protection against heart
disease. Testosterone is also responsible for normal growth and
development of male sex organs and maintenance of secondary sex
characteristics. Secondary sex characteristics are specific traits
that separate the two sexes, but are not directly part of the
reproductive system, for example: chest and facial hair, a
distinguished jaw line, broad shoulders and increased muscle mass.
Testosterone binds to the Androgen Receptors (AR), which thus causes
accelerated muscle gain, fat loss, and muscle repair and growth.
These mechanisms are stimulated by activation of the Androgen
Receptors (either directly or as DHT).
There are many possible side-effects associated with its use. This
product also has a high level of aromatization into estrogen and
coverts to DHT (dihydrotestosterone) as well. Conversion to
estrogen, the female sex hormone, creates a high risk of
gynecomastia (formation of breast tissue in males) and water
retention.
Supplementing Testosterone into your body will result in the
shutting down of the body's natural production of the hormone. The
severity of side effects depend mostly on the dose and duration of
circulating free testosterone and its conversion to substrates.
Testosterone's anabolic/androgenic effects are dependant upon
dosage, therefore, the higher the dose the higher the muscle
building effect. Testosterone also promotes aggressive and dominant
behavior.
Testosterone is possibly the best mass builder known to man and
recommended as the base of any mass building cycle.
Technical Data
Testosterone's anabolic/androgenic effects are dependant upon the
dose administered; usually th e higher the dose, the better the
results. In a study done on Testosterone (Enanthate), a dose as high
as 600 mg's (per week) produced better results in subjects compared
to those who received lower doses. At the highest dose, 600 mg/week,
the greatest results were achieved in comparison to any of the lower
doses studied. The highest fat loss, most muscle growth, and
increased size and strength were achieved at the higher dose. In the
same study, HDL cholesterol was lowered and the subjects experienced
acne. There was roughly a 15% gain in Lean Body Mass from 20 weeks
of 600 mg/week of Testosterone therapy. e higher the dose, the better the
results. In a study done on Testosterone (Enanthate), a dose as high
as 600 mg's (per week) produced better results in subjects compared
to those who received lower doses. At the highest dose, 600 mg/week,
the greatest results were achieved in comparison to any of the lower
doses studied. The highest fat loss, most muscle growth, and
increased size and strength were achieved at the higher dose. In the
same study, HDL cholesterol was lowered and the subjects experienced
acne. There was roughly a 15% gain in Lean Body Mass from 20 weeks
of 600 mg/week of Testosterone therapy.
Overall, the most common report by subjects using testosterone was
immense gains in strength as well as alterations in size, shape, and
appearance of the muscle.
Due to stimulation of the Androgen Receptors (either directly or as
DHT), accelerated muscle gain, fat loss, increased muscle repair and
growth was experienced. Testosterone binds to the A.R. on fat cells;
therefore, adipose (fat) tissue can be broken down more readily
while new fat formation is prevented. Since the body is building
muscle at an accelerated rate, more ingested food is shuttled
directly to the muscle tissue (this is known as nutrient portioning)
and away from fat. This is another indirect effect of testosterone
on fat loss. Testosterone also promotes glycogen synthesis, which is
activated by insulin in response to high glucose levels. Glycogen
provides fuel to the muscle; therefore endurance and strength
increases were reported during severe muscle breakdown in intense
training and workouts.
|

 |